RH1507: NEUROLOGIC DISORDERS: PART 6
Neurotrauma:
Traumatic Brain Injury
Cynthia Blank-Reid, Ellen Barker
The abuse of prescription drugs, illegal drugs, and alcohol significantly complicates the assessment and management of a patient with TBI. Early response by highly trained emergency medical service (EMS) personnel with early intubation and rapid transport to the hospital for definitive care has helped to reduce prehospital mortality. Aggressive resuscitation at trauma centers, early computed tomography (CT) scanning, improved intensive care monitoring, and treatment by a multidisciplinary team have resulted in decreased hospital morbidity and mortality.
Despite all these efforts, TBI has a devastating effect on the lives of those injured and on their families. The resulting disability causes a significant loss of productivity and income potential. The cost to society is more than $30 billion annually. Estimates of the average lifetime cost for an individual with severe TBI ranges from $600,000 to $1,875,000.10 The social costs may include family stress and disruptions; an increased risk for suicide, divorce, and substance abuse; economic hardships; unemployment; and a burden on community, state, and federal agencies. Thus TBI is a serious public health problem that mandates continuing efforts in the areas of prevention and treatment.
Refer to RH1500 for a review of the anatomic structures and normal physiology of the brain. This chapter focuses on
INCIDENCE
TBI occurs three times more often in males than in females. The average age of a TBI patient is between 15 and 30 years.13 TBI crosses all lines of race, religion and socioeconomic status, but the majority of patients tend to come from low-to median-income families and often do not have health insurance. The peak occurrence of TBI is during evenings, nights, and weekends.
ETIOLOGY
Injuries are usually classified by their mechanisms (e.g., blunt or penetrating) and by the type of injury (e.g., focal, diffuse, or fracture). The mechanism of injury is the event that caused the injury. Certain mechanisms of injury are associated with specific patterns and may be used to predict the severity of injury. Patients with TBI are injured from either a blunt mechanism, a penetrating mechanism, or a combination of both. Although the most common mechanism of injury associated with TBI is blunt force, neurotrauma cannot be discussed without mentioning penetrating injuries.7,25
Blunt Injuries
Blunt trauma can result from many different causes. The majority of blunt TBI occurs from the following:
The mechanism of injury affects outcome and can result from the following:
Deceleration forces: Injuries result when an individual’s head strikes an immovable object, such as the dashboard of a car.
Acceleration forces: Injuries occur when a moving object (e.g., baseball bat) strikes an individual’s head.
Acceleration-deceleration forces: Injuries often occur in combination because of the rapid changes in the velocity of the brain within the cranial vault.28,29
Rotational forces: These forces refer to the movement of the brain in a side-to-side, twisting manner inside the cranial vault. Rotational injuries often occur in combination with acceleration / deceleration injuries and result in tension and shearing of the brain tissue.
Deformation forces: These injuries are usually the result of direct blows to the head that change the shape of the skull. Such injuries result in a compression of brain tissue. The velocity of the impact determines the extent of deformation and the subsequent injury.28,29
Penetrating Injuries
A penetrating TBI can be caused by many things such as impalement injuries, nail guns, gunshot wounds (GSWs), and stab wounds (SWs). GSWs are the most lethal of all injuries to the brain, with a mortality rate of more than 90%.6,7 The pathophysiology of cranial missile injuries is based on three primary events that occur at impact 6,7:
Low-velocity
injuries
Local parenchymal damage along the bullet path is the most important factor
in determining the extent of injury. If the bullet has insufficient energy to
exit the skull, it may ricochet off the inner table opposite the entry site
or off a dural barrier such as the falx or tentorium, creating a second and
occasionally a third track. The course of such a rebounding bullet is highly
unpredictable.7
High-velocity
injuries
As the impact energy of a
missile increases, temporary cavitation and shock wave effects take on increasing
significance in determining the ultimate extent of injury. If the missile transgresses
vital brainstem structures, the patient usually dies instantaneously. Even without
anatomic disruption of the brain’s vital centers, the shock waves themselves
can be severe enough to produce transient or permanent medullary failure with
cardiopulmonary arrest.7
With GSWs to the brain, several secondary phenomena can occur and can lead to death. The pressure wave associated with a bullet that enters the skull can cause distant cerebral injuries such as cerebral contusions and marked increases in intracranial pressure (ICP); such injuries can cause uncal and tonsillar herniation. The mechanism of elevated ICP after a cranial GSW in the absence of hematoma formation is not entirely clear. The blast effect may damage cerebral vessels and may impair autoregulation. The blood-brain barrier may be damaged by the shock wave, leading to vasogenic edema. Respiratory arrest may lead to cerebral ischemia, cell death, and cytotoxic edema.
Laceration of major cerebral vessels may result in hematoma formation or the development of a traumatic aneurysm. Local parenchymal damage causes the release of tissue thromboplastin and plasminogen and may result in a consumptive coagulopathy. Multiple in-driven bone fragments can create additional areas of brain destruction. Finally scalp, hair, clothing and other foreign debris may be pulled in by the bullet, providing multiple sites for infection.
Stab wounds
Stab
wounds to the head
are less common than GSWs in the United States but are more common in countries
where guns are not readily accessible. Most stab wounds occur on the left side
of the brain because most assailants are right-handed. Neurologic symptoms arise
from vessel laceration with hematoma formation, laceration of the brain parenchyma,
or cranial nerve injury. Dysphagia is also very common given the predominance
of left hemisphere injuries. Traumatic aneurysm formation, carotid-cavernous
fistula, and arteriovenous fistulas occur in approximately half of all SW patients.7
PATHOPHYSIOLOGY
TBI can be categorized into
(1) scalp lacerations and abrasions,
(2) skull fractures,
(3) cranial nerve injuries,
(4) mild injuries, and
(5) moderate to severe injuries.
The mechanisms of injury previously described emphasize the complexity of head injury and the damaging effect that can occur to brain tissue, especially the cellular components and namely the neurons. Besides injury to the cranium, damage may occur to the scalp (which is very vascular), the bony cranial vault that protects the brain, brain parenchyma, meninges, cranial nerves, cerebral vasculature, and ventricular system.
An understanding of the pathophysiology of TBI has greatly increased during the past two decades. All neurologic damage does not occur at the moment of impact—it is a process. The primary injury is defined as the immediate biochemical effects that result from the initial trauma. Primary head injuries include the following:
Although some degree of irreversible damage occurs at the initial or primary injury, TBI is a process in which additional and progressive secondary injury evolves over the minutes, hours, and days following the primary injury. A secondary brain injury is anything that worsens the morbidity and mortality from the TBI.8,35 Secondary injuries occur as a complication of the primary injury and are a devastating consequence of the body’s physiologic mechanisms. Clinical management is focused on adequately resuscitating the patient and on preventing and/or minimizing the secondary injuries that accompany the initial injury.6,8,14 As the number, frequency, or severity of secondary injury increases, the prospect of a favorable outcome decreases. Examples of secondary injury are listed in Box 13-1.
| Box 13-1 Examples of Secondary Brain Injury |
|
To discuss every complication or situation that can cause secondary injury is
beyond the scope of this chapter. The publication of the “Guidelines
for the Management of Severe Head Injury” by the Brain Trauma Foundation
(BTF) and the American Association of Neurological Surgeons
(AANS) provides recommendations for practice based on extensive
literature reviews.8 The purpose of this document was to use evidence-based
medicine to demonstrate what was and was not effective in the treatment and
prevention of secondary injury.
Scalp Lacerations and Abrasions
The scalp is composed of three layers: dermis, subcutaneous tissue, and galea. The subcutaneous tissue is very vascular and is responsible for the profuse bleeding that usually occurs with scalp injuries. Scalp injuries can be classified as lacerations or abrasions. Important scalp laceration and abrasion considerations are shown in Boxes 13-2 and 13-3.
|
Box 13-2 Characteristics of Scalp Lacerations |
|
|
Box 13-3 Characteristics of Scalp Abrasions |
|
Skull Fractures
The skull has three layers:
The inner and outer table are hard layers of bone, and the diploë consists of cancellous or spongy bone. The skull is very hard and requires a significant amount of force to be fractured. Different types of skull fractures—including
are described in Box 13-4 and in
Figs. 13-1 , 13-2
and 13-3.
| Box 13-4 Types of Skull Fractures |
|
Linear Skull Fracture Mechanism
of injury:
Occurs secondary to a force applied over a wide surface area |
|
Basilar Skull Fracture Mechanism
of injury:
Usually caused by a direct blow to the base of the skull |
|
Anterior Fossa Fracture Location:
Usually involves frontal bone, ethmoid, and frontal or paranasal sinuses |
|
Middle Fossa Fracture Location:
Usually involves fracture of the petrous bone |
|
Depressed Skull Fracture Mechanism
of injury:
Occurs when the bones of the skull are forcefully displaced downward;
varies from a slight depression to displacement of the outer table below
the level of the inner table20 |
|
Comminuted Fracture Mechanism
of injury:
Occurs from multiple linear fractures with a depression at the site of
impact; originates and radiates toward the site of impact and toward the
base of the skull20; referred to as “eggshell
fractures” because the appearance of the skull is similar to that
of a cracked eggshell6 |
The assessment of skull fractures is related to the type, extent, location, and signs and symptoms that accompany the fracture. A focused neurologic assessment is needed to determine the impact of the fracture on the underlying brain tissue, whether the fracture was from a blunt or a penetrating force, if the fracture required surgery or bone replacement with cranioplasty, and if there is evidence of any complications (e.g., cerebrospinal fluid [CSF] leak, infection, and brain swelling) associated with the fracture. Treatment is specific to the type of fracture and the need for surgery and patient follow-up.
Cranial Nerve Injuries
The 12 pairs of cranial nerves are often involved in TBI from direct injury, compression from edema, or stretching during periods of increased ICP (see RH1506). A careful and thorough assessment of the cranial nerves should be performed at frequent intervals following TBI. Treatment may focus on the primary injury, such as hemorrhage that can irritate or cause cranial nerve compression, edema that compresses the nerves, or trauma that directly injuries or destroys the nerves. Treatment focuses on relieving the compression or surgery to reattach or repair the nerves. Careful follow-up cranial nerve assessment is needed to evaluate the patient’s response to therapy. Box 13-5 provides a full review of cranial nerve injuries.
|
Box 13-5 Cranial Nerve Injuries |
|
There is a potential for unilateral or bilateral cranial nerve injury. The exact site and orientation of the fracture determine the damage. CN I: Associated with anterior fossa fracture; results in anosmia CN II (rarely injured): Usually causes visual field cuts CN V, VI, VII, VIII: Usually associated with petrous bone fractures CN IX, X, XI, XII (rarely injured): May be involved in fractures of the posterior fossa involving the occipital condyle CN VII and VIII: Occurs secondary to fractures when the cervical spine is forced upward and impacts on the base of the skull; fracture may transverse the foramen magnum6; can result in peripheral facial palsy and in hearing deficits |
Mild Brain Injury
Concussion
A concussion,
which is often referred to as mild traumatic brain injury
or diffuse injury to the brain, is a limited disruption
of the reticular activating system (RAS) with microscopic bruising
of the brain but without a structural defect.11,18 The mechanism
of injury is usually blunt trauma from an acceleration / deceleration force
or a direct blow. The patient with a concussion may or may not give a history
of a short period of unconsciousness. Loss of consciousness may last less than
30 minutes and be followed by posttraumatic amnesia, which usually lasts less
than 24 hours.
Concussions are classified as either mild and classic. Mild concussions are characterized by cortical dysfunction related to attention span and memory without the loss of consciousness that results from temporary axonal disturbances.6,7,18 The symptoms of mild concussion span from momentary confusion and disorientation to confusion that last several minutes and is accompanied by anterograde and retrograde amnesia. Box 13-6 lists the common postconcussion symptoms.
|
Box 13-6 Common Postconcussion Symptoms |
|
Headache: Most common complaint possible from nerve fiber damage, abnormal cerebral circulation, or neurochemical changes (Some patients develop migraine headaches.) Dizziness: Secondary vestibular changes Confusion: May result from electrochemical dissociation Nausea / vomiting Hearing loss / tinnitus or phonophobia: sensitivity to sound due to impairment of CN VII and VIII Loss of smell / appetite: CN VII involvement Visual changes: Photophobia, blurred vision, impaired extraocular motor (EOM) function Speech problems: Slurred speech from mild brain damage Balance and coordination difficulties: Dislodging of calcium carbonate crystals of the semicircular canal Problems with cognitive function: Lack of concentration, short-term memory loss from mild brain damage, axonal fragmentation Emotional and behavioral changes: Irritability, poor attention span Seizures (rare): Transient absence or partial seizures with staring spells, memory gaps, and outbursts of temper that improve with anticonvulsants |
Signs and symptoms of mild brain injury
The characteristics of classic concussions may involve the following:
Symptoms of PCS include headache, dizziness, irritability, emotional lability, fatigue, poor concentration, decreased attention span, memory difficulties, and intellectual dysfunction that may occur from 1 week to 1 year after the initial injury. Patients at high risk for PCS should be identified, and they and their family should be educated about PCS so that all parties involved understand that they are not completely recovered when they leave the hospital. Sequelae may include difficulty at work and at home and may result in interpersonal relationship problems or the loss of employment.19,23,28
Patients who have not recovered 6 months after the injury require a referral for further diagnostic workup and treatment and possibly neuropsychologic testing.
With a mild brain injury, an alteration in consciousness may occur without localizing signs. The mechanism of injury may result from a severe acceleration/deceleration force or blunt trauma to the head. The location is usually in the frontal and temporal lobes, at the poles, around the sylvian fissure, at the orbital areas and, less commonly, at the parietal and occipital areas (which are more prone to brain lacerations). The difference between concussions, contusions, and intracerebral lacerations is severity, with lacerations being more serious.
Moderate to Severe Brain Injury
Contusions
Cerebral contusions are diffuse
and are a more serious TBI. They may be described as diffuse or as follows:
The effects of injury related to contusions (i.e., hemorrhage and edema) peak after about 18 to 36 hours.6,31 Contusions are characterized as moderate to severe head injuries. They are characterized by loss of consciousness associated with stupor and confusion. Patient outcome depends on the area and severity of the injury.
Temporal lobe contusions carry a greater risk for swelling, rapid deterioration, and brain herniation.10 Many of these patients fall into what has been called the “talk and die” category—they have a period of improvement after injury followed by rapid deterioration and death. This outcome can be avoided with close observation and early surgical intervention.6
Contusions located in the deeper structures of the brain (e.g., basal ganglia, corpus callosum, thalamus) are usually associated with diffuse axonal injury and carry a poor prognosis.6 These deep contusions are more often associated with hemorrhage and destruction of the reticular activating fibers for arousal.
Coup and contrecoup injury
Movement of the brain within the cranial confines causes both
contusions and lacerations. These injuries are often referred to as coup or
contrecoup injuries (Fig. 13-4).
A coup injury occurs when the damaged area forms directly at the site of impact.
A contrecoup injury occurs at the opposite side the injury because of the movement of the brain within the skull. Contrecoup injuries are usually more severe. The size of the area of impact affects the severity of the injury. The smaller the area of impact, the greater the severity of injury because of the concentration of force in a smaller area.
Diffuse Axonal Injury
Diffuse axonal injuries
(DAIs) result from widespread shearing and rotational forces
and produce damage throughout the brain. The injured area is diffuse, and there
is no identifiable focal lesion.3,28 DAIs are associated with prolonged
traumatic coma, are more serious, and have a poorer prognosis than a focal lesion
or ischemia. They have many synonyms, including shearing injury, grade V cerebral
concussion, contusion cerebri, diffuse neuronal injury, and stretch injury.29
DAIs may be described as follows:
DAIs are commonly located on the corpus callosum and the brainstem.6 Patients present with an immediate loss of consciousness followed by a prolonged coma, abnormal posturing, increased ICP, hypertension, and elevated temperature.6 The mortality rate is 33%, with another 33% surviving with severe disabilities or remaining in a persistent vegetative state.6 DAIs create an increase in vasodilation and cerebral blood volume that precipitates increased ICP over time.20
Microscopic lesions are not seen on the CT scan.6 They may appear on the CT scan as small areas of hemorrhage caused by the tearing of small blood vessels that occurs with shearing injuries.
DAIs are classified as mild, moderate, and severe:
Mild: Consists of loss of consciousness lasting 6 to 24 hours; occurs in only 8% of all severe head injuries6
Moderate: Consists of coma lasting less than 24 hours with incomplete recovery; represents 20% of all severe head injuries and 45% of all DAI injuries; often occurs with basal skull fractures
Severe: Occurs in 16% of all severe head injuries; usually involves primary brainstem injury
Brainstem Injury
Brainstem injuries may be caused by contusions or lacerations and are usually associated with other diffuse cerebral injuries. The prognosis associated with these injuries is poor due to the brainstem’s control of vital functions.22 Primary insult to the brainstem produces immediate dysfunction. The dysfunction may also appear in association with other TBIs as a result of secondary injury. Brainstem injuries produce an immediate loss of consciousness, pupillary changes, and posturing, along with cranial nerve deficits and changes in vital functions (e.g., respiratory rate and rhythm).1,2 Brainstem injuries are also classified under diffuse axonal injuries.
Focal Brain Injury
Focal injuries account for about half of all head injuries. They are the direct result of trauma to the tissue. In contrast to a diffuse brain injury, a focal brain injury is a localized injury and is limited to a specific, well-defined area. It is the direct result of trauma to the tissue (e.g., contusion, laceration, or intracerebral bleed).
Subarachnoid
hemorrhage
A subarachnoid hemorrhage (SAH) is the presence
of blood in the subarachnoid space, which lies between the arachnoid and pia
meningeal layers. When SAH occurs with trauma, it is often an incidental finding
associated with other injuries. The patient’s CSF is bloody. If the patient
is conscious, he or she may exhibit signs of meningeal irritation such as a
headache.25 Other types of cerebral hemorrhage are discussed in the
following sections.
Hematoma
Three main types of hematomas result from trauma:
One third to one half of all TBI patients develop some type of hematoma. One in four patients with skull fractures develop a surgically significant hematoma. The development of a hematoma should be explored if there is any change in LOC. Mortality rates vary according to the type of hematoma, with a subdural hematoma having the highest mortality rate.3,4 Hematomas are often associated with a cerebral contusion.
Epidural
hematoma
Epidural
hematomas (EDHs)
account for approximately 1% to 2% of all TBIs and for 20% to 30% of all hematomas.1,2,28
The persons most affected are those in the 20- to 40-year age-group. The mortality
rate is approximately 8%—the lowest of all hematomas.28
EDHs develop from bleeding into the epidural space between the skull and the dura mater. The middle meningeal artery runs through a groove in the temporal bone (the thinnest bone of the skull) and is covered by a large muscle mass. A fracture in the temporal bone may cause a tear in the middle meningeal artery, resulting in an EDH.6,28
Venous epidural hematomas can occur but are rare and occur from fractures associated with the sagittal or transverse sinuses, which result in venous bleeding.
Posterior fossa epidural hematomas are associated with fractures across the transverse sinus and constitute approximately 1% to 2% of all EDHs.6 Because of their positioning, posterior fossa epidural hematomas may cause rapid compression of the brainstem; therefore early operative intervention is necessary to prevent herniation and death.6
EDHs are initially characterized by a brief loss of consciousness. This is followed by a lucid interval in which the patient is awake and conversant. The patient then becomes increasingly restless, agitated, and confused; this condition progresses to coma. Herniation is a potential complication of EDH; the most common type of herniation syndrome associated with EDH is uncal herniation.6,28
With EDHs, an early operative intervention is associated with a more positive outcome.28 After surgery, 80% of patients have a rapid recovery with little residual neurologic deficit.6
Subdural hematoma
Subdural hematomas (SDHs)
are the most common type of hematoma and occur in approximately 10% to 20% of
all TBIs. They have the highest mortality rate.28 SDHs develop from
bleeding into the subdural space between the dura mater and the arachnoid, which
is usually the result of a rupture of the bridging veins that cross the subdural
space.29 SDHs are most commonly found around the top and sides of
the head and are associated with contusions and intracerebral hematomas. They
occur bilaterally in 15% to 20% of cases.28
There are three types of SDH:
Intracerebral
hematoma
Intracerebral hematomas can
best be described as large, focal, intraparenchymal contusions. They are considered
mass lesions when they are 25 ml or larger. Approximately 2% to 3% of these
hematomas are associated with actual contusions.1,2,18 They are caused
by penetrating injuries (e.g., gunshot wounds, stab wounds, or lacerations of
tissues), deep- depressed fractures, and DAI.6,7 Intracerebral hematomas
develop deep within the hemispheres from contused areas that become confluent
and are surrounded by edema.
Summary
of focal injuries
Lesion size and the patient’s
overall status dictate treatment. The hematoma must be evacuated if it is large
or if the patient’s neurologic status is deteriorating.6 Hematomas
act as mass lesions and are often accompanied by progressive edema, producing
a steady deterioration in the patient’s condition. This deterioration may occur
immediately or be delayed from 72 hours to 7 to 10 days.6 Clot formation
and deterioration within a few days after initial insult is called a delayed
traumatic intracerebral hematoma (DTICH).3 DTICH
occurs in the areas that were injured at the time of impact but appeared normal
on the initial CT scan. DTICH is associated with a high incidence of increased
ICP and a poor prognosis.24 There is a higher risk of development
of DTICH in patients with disseminated intravascular coagulation (DIC),
hypotension, alcohol abuse, and hypoxia.
ASSESSMENT
Initial Assessment
Prehospital providers are valuable sources of information about the patient’s status at the trauma scene, the mechanism of injury (e.g., starring of the automobile’s windshield, ejection from the vehicle, fall from a balcony), the emergency care provided, and the patient’s condition during transport. Advanced trauma life support (ATLS) guidelines and hospital head trauma protocols are immediately implemented. Guidelines from the Brain Trauma Foundation are illustrated in Fig. 13-6.
The initial assessment in the emergency department becomes the baseline against which to compare subsequent serial neurologic examinations to evaluate the patient’s condition for deterioration or improvement.
Airway (A),
breathing (B), and
circulation (C) are the immediate priority as the trauma team members quickly complete the initial assessment.
Disability (D) of any neurologic function is noted, and total
exposure (E) of the patient by removing or cutting away all clothing allows the trauma team to assess the entire body for injuries.
Simultaneously, the vital signs are obtained and provide information to the clinician about potential hypoxia, hypotension, or other factors that may influence the patient’s neurologic examination. TBI is not usually a cause of hypo-volemic shock; therefore other causes of blood loss need to be ruled out before assigning TBI as the cause.
A trauma flow sheet serves to document the initial and serial assessments. The medical record is a legal document and a communication tool by which members of the team review and observe for trends and changes that require immediate response. Therefore careful, accurate, timely, and legible charting is essential.
Clinical pathways bring the standard of care (SOC) to the patient’s bedside and function as a documentation tool that demonstrates the SOC and functional patient outcome along a time line. The clinical responsibility for each professional discipline is described in clearly measurable outcomes. The advantages of clinical pathways include the following35:
A clinical pathway should be initiated on admission. If a patient does not have an issue with a category, it is marked as nonapplicable. If a step indicated on the pathway is inappropriate at that time, it is marked as an issue to be readdressed in several days (but no longer than a week). In addition to the pathway, all trauma patients should be discussed weekly during multidisciplinary rounds to review their progress, set short-term goals, and reevaluate long-term goals. Patients who experience complications or fail to recover as predicted are considered a variance and require an explanation (Fig. 13-7).
FIG 13-7
|
Category / System |
Admission to 24 Hours |
24 Hours to 48 Hours |
49 Hours to 72 Hours |
|
Cardiopulmonary |
DVT Prophylaxis
(includes TEDS and SCDs) |
------------------------------------>
Assess airway clearance and readjust interventions as needed |
------------------------------------>
------------------------------------> |
|
Neurological |
Evaluation of
C-spine completed and findings documented in chart----------> |
If patient wearing
collar: Skin integrity under collar assessed and skin care initiated |
Vertebral
injury stabilized |
|
GI and Nutrition |
Feeding route established----------> |
Nutrition Orders
Initiated: |
Nutrition
assessed and adjusted: |
|
Infection Control and Pain Management |
Pain medication
ordered: Epidural, PCA, IM, PO |
Pain medication
adjustment based on pt. comfort level |
------------------------------------>
------------------------------------> |
|
Musculoskeletal and Skin Integrity |
Documentation
on chart: Injuries, definitive plan for fracture stabilization, plan
of care on chart |
If patient has not
been stabilized: Time frame given for comfort level. |
PM
and R’s recommendation for anticipated discharge disposition identified
based upon evaluation |
|
Psychosocial
and Discharge Planning
|
Patient identified
and next of kin notified |
Psychosocial needs
identified and resources contacted (Substance / Domestic Abuse counseling
initiated) |
Referrals
for appropriate level of care: |
|
Patient
Name: _____________________________
Medical Record Number: ____________________ Note: This pathway represents guidelines only. Physician practice may vary based upon individual patient needs. Acceptable medical practice generally does include a variety of responses to a particular clinical problem. Peer Review Records: Confidential pursuant to the Peer Review Protection Act, 63 P.S. 425.1 et. seg. and Health Care Quality Improvement Act, 1986 |
EXPECTED OUTCOMES AT 72 HOURS Hemodynamic stability Patent airway and ability to clear secretions Intake that meets metabolic needs to recover |
A comprehensive discharge plan that identifies:
|
|
| Fig. 13-7 Trauma pathway. (Courtesy Medical College of Pennsylvania Hospital, Philadelphia, Penn.) |
Secondary Assessment
The secondary survey follows the initial assessment of the patient. This assessment includes gathering additional information such as a detailed history of how the injury occurred, prehospital care, and any medical history (medications, allergies, surgeries, comorbid conditions) that may impact patient management. A more complete neurologic examination becomes part of the general systems assessment as the patient is provided ventilation and oxygenation and is closely monitored for hypoxia, cardiac dysrhythmias, and adequate perfusion. At this time the patient should have pulse oximetry, large-bore intravenous (IV) access with warmed fluids, and an indwelling urinary catheter. Blood samples are drawn for routine laboratory values and for toxicology and blood alcohol levels (BALs).
Very early after admission to the emergency department, attention is focused on appropriate management for the prevention of secondary brain damage, such as hypoxia where the patient exhibits apnea or cyanosis and a partial pressure of oxygen in arterial blood (Pao2) < 60 mm Hg, hypotension with a systolic blood pressure < 90 mm Hg, increased ICP with a surgical lesion or edema demonstrated on CT, or metabolic abnormalities.
Level
of consciousness
The most important assessment of the patient with TBI is
level of consciousness (LOC), followed by pupillary assessment
and assessment of the extremities for lateralized weakness or loss of function.
As the trauma team completes the initial assessment, the patient is preliminarily
categorized as having mild, moderate, or severe TBI. A mini neurologic examination
can be rapidly performed using the AVPU scale to determine if the patient is:
A Alert
V Responding to vocal stimuli
P Responding only to painful stimuli
U Unresponsive to all stimuli
The most widely used tool to assess a patient’s LOC is the Glasgow Coma Scale (GCS). Since its introduction in 1974, the GCS has become the tool most used to objectively score patient eye opening, motor response, and verbal performance to external stimuli. (See RH1501 for a discussion of GCS.) The highest GCS score is 15, which is normal. Any score less than 15 is considered abnormal. A score of 13 to 14 indicates a mild TBI, 9 to 12 a moderate injury, and 8 or less a severe head injury.1,2,3
Pupillary
changes
Pupillary changes range from a decrease in reactivity to bilateral fixation
and dilation. (See RH1501 for
pupil assessment.) Pupil changes indicate increased ICP resulting in CN III
compression, as well as injury or ischemia to certain areas of the brain. The
pupils are normally round, approximately 3 to 5 cm in diameter, equal in size,
and briskly reactive to light. Several factors can influence the size, shape,
and reactivity of pupils, such as a history of a previous ocular injury, alcohol
ingestion, or the use of certain medications or illicit drugs.1,2,3
A pupil that is oval in shape indicates increased ICP and CN III compression and develops into a fixed and dilated pupil if left untreated. This is seen most often in severe closed-head injuries.4 Bilaterally fixed and dilated pupils indicate massive elevations in ICP, which can result in brain death. A metabolically induced coma does not affect pupillary reaction (Fig. 13-8). Changes in pupil size, shape, and reactivity may indicate rising ICP and should be reported to the physician immediately.1,2,3,20
Brainstem
reflexes
Several reflexes that originate in the brainstem that should
be assessed. These reflexes include the cough, gag, corneal, doll’s eyes, oculocephalic,
cold calorics, and oculovestibular reflexes (see RH1500
and RH1501). These reflexes test
CN V through CN X. The presence of these reflexes indicates that the integrity
of the brainstem has not been disrupted.2 An absence of these reflexes
signifies a poor prognosis.
Vital
signs
Vital sign changes are a late indication of increased ICP.
Cushing’s reflex is seen in approximately
75% of patients with increased ICP and is a triad of late symptoms involving
vital sign changes that indicate decompensation of the brainstem.2
These changes include an increase in systolic blood pressure, a widening pulse
pressure, and bradycardia. Patients with TBI and increased ICP show a reduced
variability in heart rate regardless of activity. The vital signs must be routinely
monitored; although the immediate response to TBI is an increase in blood pressure
and ICP, these variables should return to normal within 1 to 2 minutes.20
Blood pressure is often decreased with severe injuries and indicates a poor
prognosis because of the negative effect on cerebral perfusion pressure (CPP).20
A decreased blood pressure in the presence of increased ICP results in inadequate
CPP, which precipitates further neuronal tissue damage from ischemia and a further
increase in ICP. Systemic hypertension can also have deleterious effects on
perfusion pressure. Hypertension increases cerebral blood flow, which in turn
increases ICP and results in an inadequate CPP. Increased blood pressure may
increase cerebral blood flow but, if autoregulation is intact, cerebral vasoconstriction
will occur to control volume.20
Cardiac
changes
Intracranial injuries can produce changes in cardiac rate,
rhythm, and conduction, and these changes may be neurogenic in origin.34
Different intracranial lesions are associated with different cardiac changes.
Atrial fibrillation and bundle branch blocks are associated with contusions.
A subdural hematoma (SDH) may produce conduction defects as
well as atrial and ventricular ectopy. Junctional escape rhythms, progressive
bradycardia, and idioventricular rhythms are seen more often with hemorrhages
and increased ICP. ST- and T-wave changes occur with severe TBIs.31
Neurogenic T waves (inverted T waves of increased amplitude and duration) are
seen in a variety of neurologic diagnoses. There are little data to explain
the cause of these changes, but they are thought to be related to the catecholamine
response that occurs after injury.31 Because of the nature of these
disease processes and their concurrent changes, continuous ECG monitoring is
essential in patients with severe TBI.31
Respiratory
changes
Respiratory rate and rhythm changes also occur in neurologically impaired patients.
Cheyne-Stokes respiratory patterns are associated
with damage to the bilateral hemispheres and the basal ganglia and often precede
cerebral herniation. Central neurogenic hyperventilation (CNH)
may occur as a compensatory mechanism to increased ICP. Hyperventilation reduces
the PaO2, resulting in vasoconstriction of cerebral vessels and reduced
ICP. CNH is also associated with damage to the midbrain and pons.6,20
Apneustic breathing is characterized by a prolonged
inspiration followed by a pause and then a short expiratory phase. This also
is associated with pontine injury. Ataxic or agonal respirations
are associated with medullary damage and may progressively deteriorate to apnea.
The clinician should be able to identify changes in a patient’s respiratory
pattern, because these changes are often indicative of deterioration. Early
detection of respiratory pattern changes and immediate, appropriate intervention
prevents hypoxia, which contributes to secondary brain damage.6
Temperature
changes
Temperature changes occur rapidly and are common in the
TBI patient population. Ongoing monitoring is essential in preventing hyperthermia
and hypothermia. Hypothermia has been defined as a core body temperature of
less than 35° C (95° F). Hypothermia results when the body
can no longer maintain an adequate temperature. It needs to be rapidly recognized
and treated for life-threatening complications such as apnea, ventricular fibrillation,
and acidosis.17,33
Hypothermia is common with trauma patients as a result of environmental exposures, stress, and the administration of unwarmed IV fluids and blood products to correct massive hypovolemic shock. Age also plays a role in hypothermia, with older adults more at risk because of their high incidence of cardiovascular disease and decreased body fat. In addition, the patient’s ability to shiver can be affected by medications (e.g., phenothiazines, neuromuscular blocking agents), an elevated BAL, traumatic injuries, hypovolemic shock, and diseases such as diabetes. Active and passive rewarming are absolutely necessary in order to keep patients from becoming hypothermic.17,22
Hypothalamic damage as well as infection often cause temperature increases. Hyperthermia increases the metabolic demands and oxygen consumption in an already overtaxed system. Oxygen consumption increases 10% for every degree of temperature elevation. Increased temperatures cause increased cerebral metabolic activity, increased CBF, and increased carbon dioxide production, all of which increase ICP.33 Elevations above 38° C should be treated rapidly.33 Elevated temperatures related to the neurologic injury and not to an infection may be refractory to acet-aminophen and aspirin. Other cooling methods such as cool sponge baths or hypothermia blankets may need to be instituted. Prevention, early detection, and intervention are essential in minimizing the metabolic demands on the brain. It is important to try to maintain a normothermia temperature with the use of antipyretics, antibiotics, and cooling blankets.22,33
Neurologic
deficits
Neurologic deficits are evaluated by completing and recording the neurologic
assessment to include level of consciousness (LOC), motor and
sensory evaluations, pupils, and cranial nerves.
Pain
Pain is the fifth vital sign
and can be evaluated by asking the awake patient if he or she feels pain in
any part of the body. The extent and severity of pain is determined by using
a pain scale or, if patient is unable to report pain, by observing for facial
expressions, body movements, crying, restlessness, and an increased heart rate
or blood pressure (see RH1512).
Sedating the neurotrauma patient should be avoided until the trauma team leader
has cleared the patient to receive analgesics, because pain medications can
cause hypotension. It is difficult to determine the extent of pain in patients
who are unconscious or pharmacologically paralyzed. The clinician can use a
variety of clues to deduce the pain status of an unresponsive patient. These
clues can be determined by assessing the following:
HIGH-RISK NURSING DIAGNOSIS
NEURODIAGNOSTIC / LABORATORY STUDIES
Skull radiographs: Detects skull or facial fractures, tumors, or foreign bodies.7
CT: Best study for rapid diagnosis of type, location and extent of injury. A CT scan provides a quick comparison with serial scans and detects absent or compressed cisterns. A dual diagnosis of head and spinal injury can be ruled out with both a head and neck CT. CT images are usually repeated every 2 to 3 days after admission or as needed based on the patient’s clinical presentation.29
MRI: Allows for a better definition of mass lesions, better visualization of the posterior fossa and brainstem, and an increased ability to detect subtle changes in tissue water content. An MRI scan requires more time than a CT scan and is not usually performed in acute or unstable patients, who are at high risk during scanning.
Cerebral angiography: Has limited use with trauma unless there are suspicions of cerebrovascular disease, vessel abnormality, or injury.
EEG: Detects abnormal electrical or seizure activity and the absence of electrical potentials as part of the diagnosis for brain death.
Cerebral blood flow studies (Xenon CT, Transcranial Doppler): Provide noninvasive measurements of cerebral blood flow (CBF) velocity, the diameter of cerebral blood vessels, or the presence of vasospasm. These studies can determine whether an increase in ICP is due to an increase in cerebral blood flow or to cerebral edema.
Evoked potentials (EPs): Measure the brain’s response to auditory, somatosensory, and visual stimuli.
Infrared spectroscopy: Noninvasive assessments of oxygen saturation.
SPECT: Measures abnormalities in regional blood flow.
PET (if available): Evaluates tissue blood flow and the use of oxygen glucose.
TREATMENT
Medical Management
Medical management of the patient with TBI begins in the prehospital setting with the goal of rapid, accurate diagnosis of the primary brain injury and the prevention or management of secondary brain injuries. On-the-scene rescue efforts, rapid transportation, initial resuscitation in trauma-designated hospital emergency departments, and improved treatment within the “golden hour” are responsible for an increase in the percentage of patients who survive their initial injury.5 When the patient reaches the emergency department, resuscitation efforts continue until the patient is stabilized and transferred to the intensive care setting. The ABCDs in the following sections demand evaluation.
Airway
All patients should be evaluated for the ability to protect their
airway and oxygenate themselves and for the need for supplemental oxygen. Establishing
and maintaining an airway is crucial in patients who are at high risk for hypoxia
or aspiration. All patients with TBI who are unconscious should be treated for
cervical spine (C-spine) injuries until the diagnosis demonstrates
otherwise.29 Spontaneous, unexpected vomiting is common in these
patients 30 to 60 minutes after injury, and therefore suctioning equipment must
be readily available.29 Intubation should occur in either the prehospital
or emergency department setting for those patients with a GCS of 8 or less.29
Strategies to use in the emergency department may include a rapid sequence intubation
(RSI) protocol, lidocaine, and / or etomidate in recognition
that intubation can be a noxious stimulation to the brain and increase ICP.29
Breathing
Of those patients with severe TBI, 65% are hypoxic and have Pao2
levels below 50 mm Hg on admission to the emergency department. The use of a
flow sheet to closely monitor the patient’s respiratory pattern and rate provide
clues to an expanding lesion. Ventilated patients must be monitored for the
need to administer neuromuscular blockade agents (e.g., succinylcholine or rocuronium)
and sedatives (e.g., midazolam) to prevent asynchronous ventilation.21
Circulation
The goal is to stabilize and maintain blood pressure and cerebral perfusion
pressure (CPP). The systolic blood pressure should not fall
below 90 mm Hg,5 and CPP should not fall below 70 mm Hg. Hemoglobin
and hematocrit should be maintained at normal levels to maximize the oxygen-carrying
capacity and oxygen delivery to the brain.6 Volume expanders and
vasopressors (e.g., phenylephrine, epinephrine, or dopamine) allow for the titration
of systemic vascular resistance and cardiac output without altering cerebral
vascular tone.
Disability
Any apparent neurologic deficits noted in the primary survey, such as altered
level of consciousness, unconsciousness, unequal pupils, cranial nerve abnormalities,
and hemiplegia, should be immediately addressed on admission.
The Head Injury Guidelines
Patient management is focused on preventing or treating the increased ICP that accompanies the primary injury. Box 13-7 describes the standard therapeutic regimen for the management of head injury.8
| Box 13-7 Standard Regimen for Clinical Management of Head Injury |
|
| ICP, Intracranial pressure; Pao2, partial pressure of oxygen in arterial blood. |
Fig. 13-6 illustrates the algorithm for initial management, and Table 13-1 provides a summary of head injury guidelines from the Brain Trauma Foundation and the American Association of Neurological Surgeons.
|
Table 13-1 Summary of Head Injury Guidelines from the Brain Trauma Foundation and American Association of Neurological Surgeon |
|||
|
Issue |
Standard |
Guideline
|
Option
|
|
Trauma systems and the neurosurgeon
Indications for ICP monitoring
Nutritional support of patients with TBI
|
None
None
|
Organized trauma care systems should exist throughout the United States.
None
None
None |
Neurosurgeons should be involved in the planning, implementing, and evaluating care for patients with neurotrauma. Complete and rapid physiologic resuscitation should occur. Maintain MAP > 90 mm Hg with a CPP > 70 mm Hg.
None noted but a recommendation was made: Connecting ventricular catheters to an external strain gauge transducer or a fiberoptic transducer is the most reliable method of monitoring ICP. Maintain CPP > 70 mm Hg.
Mannitol can be used
before ICP monitoring if the patient exhibits neurologic deterioration
or transtentorial herniation; maintain serum osmolarity below 320 mOsm;
maintain fluid replacement and euvolemia.
|
|
Data from Guidelines for the management and prognosis of traumatic brain injury, a joint project of the Brain Trauma Foundation and American Association of Neurological Surgeons. ICP, Intracranial pressure; TBI, traumatic brain injury; CT, computed tomography; GCS, Glasgow Coma Scale; MAP, mean arterial pressure; CPP, central perfusion pressure; Paco2, partial pressure of carbon dioxide in arterial blood. |
|||
Other Variables That Affect Secondary Injury
Seizures
Seizures can increase
the cerebral metabolic rate, increase cerebral oxygen demand, and exacerbate
ischemic damage (see RH1512).36
Clinicians need to be aware that patients who are pharmacologically paralyzed
can still be seizing. A bedside continuous electroencephalogram (EEG)
may be used to determine if the patient is seizing. The Guidelines for the Management
of Severe Head Injury recommend that anticonvulsant therapy be initiated in
patients who are at high risk for seizures (e.g., those with a seizure history,
those who have already had a seizure as a result of their injury).8
Approximately 5000 new cases of posttraumatic seizures (PTSs) are identified each year in the United States.14 PTSs are classified into two groups:
Tonic-clonic seizures in the acute phase may cause secondary brain injury resulting from increased ICP, compromised oxygen delivery, increased metabolic demands, and excessive neurotransmitter release.9 Early seizures should be managed with IV lorazepam (Ativan) 0.1 mg / kg up to 10 mg. If seizures persist, lorazepam can be followed with a loading dose of phenytoin or fosphenytoin (Cerebyx). Fosphenytoin is a product of phenytoin sodium equivalents (PSEs). The loading dose for phenytoin is 18 to 20 mg / kg IV at an infusion rate of 50 mg / min; the loading dose for fosphenytoin is 18 to 20 mg / kg PSE IV at 150 mg / min.9 The goals of the clinician should include patient safety, timely administration of anticonvulsants, first aid for seizures (ABCs), and a thorough documentation of the seizure.
Pulmonary issues
There is a 20% incidence of acute respiratory failure in the patient with neurologic trauma.21,22 One type of acute respiratory failure is neurogenic pulmonary edema (NPE) (Box 13-8).
|
Box 13-8 Cycle of Neurogenic Pulmonary Edema in Traumatic Brain Injury |
|
Trauma
or insult to the brainstem |
|
Modified from Marshall SB et al: Neuroscience critical care: pathophysiology and patient management, Philadelphia, 1990, WB Saunders. ICP, Intracranial pressure; CO2, carbon dioxide. |
NPE appears to occur only with massive and often fatal brain injuries.11
NPE may develop minutes to hours after the initial insult and usually resolves
after 24 to 48 hours.22 NPE may be caused by a sudden increase in
ICP and the subsequent release of catecholamines. The catecholamines cause constriction
of the pulmonary vasculature, pulmonary hypoperfusion, and hypoxia. Some experts
believe NPE is a form of acute respiratory distress syndrome
(ARDS).3,22
ARDS may also occur in patients with TBI. Treatment continues to be aimed at minimizing hypoxia. Unfortunately, the treatment of ARDS and NPE conflicts with the management of ICP because of the use of positive end-expiratory pressure (PEEP), which raises the intrathoracic pressure. This increase in intrathoracic pressure is transmitted through the venous system where, due to the lack of valves in the cerebral veins, venous outflow from the brain is reduced. This reduction in venous outflow causes an increase in cerebral blood volume and therefore increased ICP.3 The desired level of PEEP is tested by observing for an increase in ICP and a change in the oxygen saturation. (See RH1506 for further ventilatory management issues.)
Other pulmonary complications may result from the trauma, such as pulmonary contusions, hemothorax or pneumo-thorax, rib fractures, and sternal fractures. The goal is to provide the brain with adequate oxygen between 80 and 100 mm Hg and to keep the Paco2 at 30 to 35 mm Hg.21
Tissue acidosis
A 40% decrease in cerebral blood flow (CBF) results in brain
tissue acidosis, and a decrease of 60% results in electrical deterioration.31
CBF may be normal, increased, or decreased after TBI. Within the first few days
after injury, there is a decrease in flow around the injured sites.6,14
This decrease causes an acidosis, which in turn dilates the vessels and causes
hyperemia. This raises the ICP, decreases CPP, and results in decreased blood
flow20,28 (Box 13-9).
|
Box 13-9 Metabolic Cascade Effects of Brain Injury |
|
Initial
brain injury (e.g., head trauma or stroke) |
| Modified from Barton R et al: The effects of brain injury, Headlines 4(1):3, 1993. |
Tip: The brain extracts more oxygen from the blood than any
other area of the body.
Jugular bulb catheterization
Jugular bulb
catheterization (Sjo2)
is an invasive procedure in which the saturation of venous blood is measured
as it leaves the supratentorial component in the upper hemisphere. Sjo2
monitoring gives the arterial-to-venous oxygen content difference (AVdo2)
and lactic acid production.20,28 This information allows patient
treatment to be individualized. Sjo2 readings below 55% are referred
to as “cerebral oligemia”; readings above 75% are
referred to as “cerebral hyperemia.” An increase
in AVdo2 that is related to an increase in CBF is better treated
with sedation and barbiturates. The ability to monitor CBF and ICP adds new
dimensions to the care of the TBI. (See RH1506
for more information on Sjo2 monitoring.)
Medullary
ischemia
Medullary ischemia appears
to be responsible for initiating a massive sympathetic discharge, which releases
catecholamines and results in increased systolic pressure, tachycardia, and
increased ICP.22 Catecholamine-blocking agents may be useful in controlling
blood pressure. Agents such as labetalol and esmolol can treat the increase
in blood pressure without affecting cerebral vascular reactivity.6
These agents should not be administered without first checking the CPP. If the
blood pressure is increasing secondary to the increased ICP, the first treatment
should be aimed at decreasing ICP to preserve and maintain CPP. Catecholamine-blocking
drugs may also be helpful in decreasing the myocardial response to the increase
in catecholamines and may be helpful in preventing myocardial ischemia.3
Cerebral edema
Cerebral edema becomes clinically significant when it results in a focal mass
effect or when it produces a global elevation in ICP and impairs cerebral perfusion.
Two types of cerebral edema can develop after TBI:
Although these two types of cerebral edema are different, both increase brain volume by increasing the water content within the brain. Regardless of the type of cerebral edema, there is an increase in ICP, a decrease in CPP, and a decrease in CBF. High CBF, called luxury perfusion syndrome, is also an indicator of a poor prognosis.3 Chemical autoregulation is extremely robust and is rarely lost except in cases of severe injury, which usually result in either death or survival in a persistent vegetative state.3,28
Surgical Management
Patients with an expanding epidural hematoma require emergency surgery for evacuation of the hematoma and cauterization of the bleeding vessel. Trauma patients with a subdural hematoma (SDH) may be managed medically when the clot is small unless the bleeding continues and a craniotomy is needed to locate and stop the bleeding (see RH1505). Patients with depressed skull fractures and other serious fractures may also be sent to the operating room (OR) for elevation of bone and repair of the dura and brain tissue. Most studies indicate that the prognosis for recovery from focal TBI is very good with early surgical intervention for mass lesions.
Once it is determined that the injury requires surgical intervention, the neurosurgeon will decide the type of procedure and the timing of surgery. Such decisions are made based on the injury. Surgery may range from burr holes to craniotomy, craniectomy, cranioplasty, or ventriculostomy.
Clinical Management
Acute care
Patients with TBI may
be admitted to the neuroscience critical care unit (NCCU) from
the emergency department or OR after resuscitation, stabilization, or surgical
repair of their injuries. Steps must be taken to reduce external stimuli by
reducing room lighting, noise levels, and frequent interruptions by the multitude
of medical staff to examine the patient. Family can be taught therapeutic touch
techniques. The goals of acute care management are to protect the brain from
secondary injury while maintaining ICP and CPP within normal limits16
(see Box 13-7).
Diuresis
Osmotic diuresis is used
to manage the excess fluid in brain tissue. Osmotic diuretics must remain
in the intravascular compartment to be effective in reducing brain swelling.
A hyperosmolar agent such as mannitol is used for osmotic therapy. Mannitol
creates an osmotic gradient across the blood-brain barrier. It increases plasma
osmolarity and pulls fluid from normal brain tissue to decrease cerebral edema.5
The usual dose is 0.25 to 1.0 g / kg IV, and
when given as a bolus it has a rapid and immediate effect—within 10 to 15 minutes.11
Mannitol decreases blood viscosity, and its effects last 2 to 6 hours.5
It is eliminated via the kidneys. Mannitol may leak into the injured brain and
pull fluid into these cells, which can result in increased ICP 8 to 12 hours
after administration. Mannitol can also have a rebound effect, causing an increase
in ICP.
The use of mannitol can cause hypertension. It is important that the patient’s vital signs be closely monitored and that an MAP greater than 90 mm Hg is maintained. This can be done with the use of albumin, normal saline, packed red blood cells (RBCs) and vasopressors.1,5
Lasix is a loop diuretic that is used as an adjunctive therapy in an effort to minimize the negative effects of mannitol. When Lasix and mannitol are used together, Lasix can do the following:
Fluid
replacement / restriction
Although it is not desirable for patients to be hypovolemic, fluid restriction
may be necessary when ICP is elevated and becoming refractory to other therapies.5
The goal of fluid restriction is to improve mean arterial pressure (MAP),
normalize CPP, and maintain euvolemia. Such therapy may be maintained for long
periods to control ICP until compliance returns to normal.11
A fluid restriction of 2 L / day is sufficient to cause mild dehydration.8 Particular attention should be given to serum sodium, potassium, and osmolarity during this therapeutic intervention.1,3,22
The replacement formula is based on the amount of diuretic therapy used, the patient’s laboratory values, and the patient’s clinical condition. Fluid replacement consists of albumin, packed red blood cells, and normal saline with potassium chloride (per protocol).
Metabolic rate
Cerebral metabolic rate can be increased 40% to 100% above normal in patients
with TBI.12 Decreasing the patient’s metabolic requirement is a priority,
because hypermetabolic states increase the production of carbon dioxide and
produce hypercarbia status, which further increases ICP.
The following measures are used to lower the patient’s cerebral metabolic requirement:
Sedation
Sedation reduces restlessness and agitation. It also decreases
the metabolic rate and rate of oxygen consumption. Lorazepam (Ativan) or midazolam
(Versed) may be required per the institution’s protocol. Opioids (narcotics)
have the advantage of being reversed to allow for the completion of an accurate
assessment. Morphine should be avoided due to its hypotensive effects. Propofol
(Diprivan) may cause agitation and should be discontinued if this occurs.2,22,26
Intubated patients may have an increase in ICP because the endotracheal tube can act as a noxious stimuli and require fentanyl (small boluses allow for pupil evaluation while decreasing the effect of noxious stimuli). Sedatives should be used very cautiously with nonventilated patients, because a decrease in respiratory rate and respiratory depression may precipitate an increase in ICP.26
Paralytic agents
The objective and guidelines for pharmacologic paralysis includes reducing skeletal
muscle activity, metabolic rate, and oxygen consumption. Paralytic agents offer
no analgesic effect and do not adequately protect the patient from noxious stimuli.
However, when used with sedatives, paralytics may help reduce the increase in
cerebral metabolic rate related to agitation. The use of neuromuscular blocking
agents (i.e., pancuronium [Pavulon], atracurium [Tracrium], vecuronium [Norcuron],
and rocuronium [Zemuron]) without sedation should never be allowed.
Alert: Pancuronium can cause tachycardia, which may necessitate the use of a beta blocker.3
When paralytic agents are used with ICP monitoring and ventilation, the patient’s corneas are protected with artificial tears, and the eyes are taped shut or a moisture chamber is applied. The standard of care requires the use of “train of four” for monitoring the level of paralysis to ensure that the smallest amount of drug is used to achieve the desired level of paralysis. (The “train of four” refers to the application of a peripheral nerve stimulator to the ulnar nerve to determine neuromuscular function.)
Barbiturate
coma
A barbiturate coma is used as therapy for hemodynamically
stable patients with severe TBI and intracranial hypertension who are thought
to be salvageable but who have been refractory to maximal medical and surgical
therapies. The diagnosis of a delayed bleed / lesion should be ruled out before
the induction of a barbiturate coma.
A barbiturate coma is a pharmacologically induced coma state that lowers cerebral metabolism and CBF. It acts as a neuroprotective therapy and decreases oxygen uptake in the brain, which decreases the cerebral metabolic rate of oxygen consumption (CMRo2) and the CBF by as much as 50%. It may also assist in stabilizing cell membranes, producing a more uniform blood supply and decreasing the formation of vasogenic edema.1,2,22
Pentobarbital is the drug of choice for barbiturate therapy because its half-life is 24 hours. It is administered as a loading dose of 36 mg / kg, with a maintenance dosage of 1 to 3 mg / kg / hr. Blood pressure and CPP may fall with the loading dose. Vasopressors, inotropes, and volume expanders may be used to help maintain systolic blood pressure and CPP.
Barbiturate infusion levels are regulated by burst suppression pattern appearance on EEG.3 The barbiturate coma is slowly decreased after the ICP is normal for 24 to 48 hours. This type of therapy requires complex monitoring, nursing care, and medical care. It is instituted only in specially equipped critical care areas.3,22
Additional assessments
A complete neurologic assessment is performed for a baseline evaluation on admission
to the NCCU. Subtle changes can be easily detected when subsequent assessments
are charted on the neurologic flow sheet to document the patient’s changing
status. The Rancho Los Amigos scale is a useful tool for identifying levels
of dysfunction and for planning the appropriate nursing interventions (see Table
13-2).27
In addition to the interventions described previously, acute care for the patient with TBI includes frequent and careful monitoring and documentation to manage the following parameters:
For patients with a GCS score of 8 or less, ICP monitoring is performed per protocol for drainage and placement of the drainage bag. For patients with a GCS score of 7 or less, hemodynamic monitoring is performed with a Swan-Ganz catheter and invasive lines. Airway clearance and respiratory rate and rhythm are monitored frequently. The cough, gag, and corneal reflexes are assessed, and the lungs are auscultated every 2 hours to detect adventitious lung sounds that may indicate respiratory failure. Intake and output (I&O) are monitored every shift.
Famotidine (Pepcid) 20 mg IV every 12 hours or and/or Maalox 30 ml PO or via nasogastric (NG) tube for a stomach pH less than 5 are administered to prevent stress ulcers.
Patients with TBI are turned every 1 to 2 hours to mobilize secretions. The use of specialty beds, when required, does not negate turning the patients.1,2 Antiembolic stockings with sequential compression devices are also used.
Suctioning should never be done through the nose, because a basal skull fracture may be present. The patient is suctioned as often as needed but at least every 2 hours. The patient is premedicated with lidocaine 0.5 to 1.5 mg / kg IV or via endotracheal tube to suppress the cough reflex and to prevent ICP elevations1,2; the patient is also preoxygenated with 100% oxygen. Suctioning is limited to two passes, and instilling saline down the endotracheal tube is avoided. Secretions are monitored for viscosity, color, and odor (a foul smell may indicate an infection). Humidified air may assist in decreasing secretion viscosity. Chest physiotherapy and postural drain-age are performed at least every 2 hours.
Prevention
of complications
Several complications are described in detail in the following sections to emphasize
their importance in preventing complications that could cause further neurologic
impairment.
Impaired gas exchange
Impaired gas exchange is managed by the following:
Increased intracranial
pressure
Nursing activities have been found to contribute to a rise in ICP.8,20
The clinician should follow the guidelines in RH1506
to prevent elevated ICP4,5,6:
For patients with a ventriculostomy, drain CSF by opening the stopcock to release a small amount of CSF, then reevaluate the patient’s ICP.
Deficient / excess
fluid volume
Deficient or excess fluid volume is managed by the following:
Imbalanced nutrition
Nutrition
must be adequate for the injured brain to heal. The following guidelines are
recommended:
Nutrition consultation: To establish a feeding route within 24 hours of admission
Enteral feeding: Preferred over parenteral12,32,34
Gastric residuals: Checked every 2 hours, with feedings slowly advanced
Daily weights
Calorie counts (when patients are able to take PO): Ensures that high caloric demands are being met
Altered elimination
Elimination
should be established early after admission. The clinician should keep the following
points in mind1,2:
Impaired
physical mobility
Patient immobility affects
all body systems. The following guidelines will help prevent complications of
immobility:
Disturbed sensory
perception
Sensory alterations are important considerations, and treatment may include
the following:
The occupational therapist may assist with a coma- stimulation program, including all types of sensory stimuli (see RH1504 for a discussion on coma). All senses—tactile, gustatory, olfactory, visual, and auditory—are stimulated. The patient should be spoken to in a calm reassuring voice, with all procedures and treatments explained.
Acute
pain
Acute pain may result from injuries sustained from the initial
injury, surgery, invasive procedures, or stimulation applied to provoke a response
(see RH1512). Considerations must
be made for the following:
Neuromuscular blocking agents should not be administered without analgesia because they have no effect on the perception of pain—only on the ability to respond to it.1,3,11,26
Ineffective thermoregulation
Temperature control issues have been discussed previously. All other
causes of fever should be evaluated for and eliminated before the cause is attributed
to neurologic damage.22,33 Tylenol 650 mg per rectum (PR)
or PO every 4 hours is administered for a temperature over 101.5°
F.
Postacute
/ nonacute care
After the patient is physiologically stable and his or
her ICP has returned to normal, he or she is transferred to a nonacute unit.
The patient is usually more awake and alert, and agitation may increase. There
are potential problems for seizure activity, injury from falls, and aspiration
as the patient starts oral feedings.
Assessment continues to play a key role. Neurobehavioral testing should be initiated2,15,19,27,28 to evaluate cognitive, adaptive, and emotional behaviors.24 These behaviors or responses reflect cortical function. Neuropsychologic testing assists in planning ongoing care, determining rehabilitation potential, and identifying realistic individual goals.15,27
The patient may need assistance to regain and build or maintain independent skills (activities of daily living), such as speaking, ambulating, eating, drinking, bathing, and performing personal hygiene to bridge the gap from dependence to independence and rehabilitation.
High-risk nursing diagnoses
Level
of consciousness (LOC)
The higher Rancho Los Amigos Scale of Cognitive Functioning
reflects the increased responsiveness that indicates recovery.15,24
The patient’s responsiveness may vary between the following behaviors:
Interventions for this increased responsiveness include a structured environment to reduce overstimulation and distraction and acknowledging behavior calmly while correcting misperceptions and refocusing the patient. The family must be included and educated on how to intercede with the patient; this will help reduce their anxiety and prepare them for the future.20,27
Physical or chemical restraints should be used judiciously and only when the patient poses a danger to himself or herself or others.27 The least restrictive interventions should be used and should include a netted bed and family and/or sitters. Someone should be with the patient at all times during periods of confusion, restlessness, and agitation to prevent the patient from getting out of bed, falling, or self-harm.
Disturbed thought
processes
The Rancho Los Amigos Scale of Cognitive Functioning assists in
selecting the appropriate actions based on the patient’s cognitive status and
abilities (Table 13-2).
|
Table 13-2 Rancho Los Amigos Scale of Cognitive Levels and Expected Behavior |
|
|
Cognitive Level |
Expected Behavior |
|
Level I
Level II
Level III
Level IV
Level VI
|
Patient is unresponsive to any stimuli.
Responses are directly
related to the type of stimulus presented but may be inconsistent. Patient is in a heightened
state of activity with a severely decreased ability to process information. Patient appears alert
and is able to follow simple commands consistently. Patient shows goal-directed
behavior. Patient appears appropriate
and oriented within familiar settings. Patient is alert and
oriented and able to integrate past and recent events. |
The following guidelines are useful:
Self-care deficits
The goals of the TBI team are based on some of the following:
The physical therapist, occupational therapist, speech therapist, and neuropsychologist should evaluate and develop a rehabilitation plan that includes weekly evaluations.
Risk for injury
The patient with a TBI can be injured as a result of the following:
Restraints are used as a last resort to keep the patient from self-harm.27 Their use should be discussed with family members, and hospital policy should be followed.
Posttraumatic
epilepsy
Posttraumatic epilepsy occurs
after TBI, with both focal and grand mal (tonic-clonic) seizures occurring.
Their incidence appears to be greater in those who experience penetrating as
opposed to blunt head injuries.7,9 The onset of posttraumatic epilepsy
varies greatly—from 1 month up to 2 years after the original injury. This condition
is best controlled with anticonvulsant therapy.9 It has a propensity
to decrease over the years, with some patients becoming seizure free.9,22
Situational
low self-esteem
Increasing the patient’s
self-esteem focuses on the following interventions:
Compromised family
coping
Like the patient, family members experience a loss of control and feelings of
fear and helplessness. Assist the family by using some of the following interventions:
COMPREHENSIVE PATIENT MANAGEMENT: TRAUMATIC BRAIN INJURY
Health Teaching
Each day patients and their family experience uncertainty, and with every health care provider they encounter questions and concerns about the injury, treatments, and outcomes. Daily and scheduled family conferences are needed to discuss the injury and the care. Family support is critical in understanding the injury and accepting the goals for each phase of care. Because family members are an important part of the health care team and usually become the caregivers, teaching should begin as soon as they indicate a readiness to learn and participate. Young males are the most likely to sustain brain injuries, with the parents suddenly becoming responsible for caring for and meeting the needs of a son who would normally be leaving home and enjoying the independence of youth. A spouse may become the major caretaker and experience a role reversal as well as become a major caregiver. A young couple may find that an older parent needs their assistance in recovering from a TBI.
The consequences of caring for a family member with TBI may impede learning until the stress decreases and the reality of the daily routine needs can be explained and demonstrated. Family members should be educated on every aspect of brain injury and rehabilitation (see Resources at the end of this chapter). A list of treatments and medications can be reviewed with the expectation that family members will be able to recognize what they can do and what follow-up can be expected from other health care providers. Insurance and benefits can be provided by social services. Case managers and life care planners (see RH1551) are often consulted for complex cases that require long-term follow-up.
Nutritional Considerations
Swallowing is a complex process that requires a great deal of cognitive function and excellent muscle coordination. Problems with eating and swallowing place the patient with TBI at risk for dysphagia. Interventions include the following:
Speech therapy evaluation: This evaluation determines the type of dysphagia and designs a plan for the patient to ensure adequate nutrition and to prevent aspiration.
Choking prevention: If the patient has trouble swallowing (i.e., chokes or gasps), oral feedings should be suspended until a dysphagia consult can be obtained.
Feeding tube maintenance: A feeding tube remains in place until the team determines that the patient is able to take in enough calories by mouth.12,32
Oral feeding: Dysphagia rehabilitation is a slow process but can be done successfully in most instances. Such rehabilitation requires tremendous patience in preventing aspiration and in allowing the patient to consume the adequate amount of food.
Psychosocial Considerations
The psychosocial dysfunction experienced by patients with TBI is perhaps the major obstacle faced after survival. Their lives and the lives of their families are altered forever. Patients and their families must cope with many stressors as they face the fear of unknown and unpredictable outcomes. Psychosocial support is needed to deal with these concerns, to help reduce stress and anxiety, and to promote adequate coping skills. Patient outcomes range from mild with no residual deficits to a persistent vegetative state, with every condition in between possible. Neurologic deficits may include impairments in language, cognition, personality, mentation, and movement. The patient is evaluated for the need for professional psychologic counseling.
Rehabilitation and education of both the patient and family must start on admission. Families require education and crisis intervention during the initial stages and support throughout hospitalization and often for an extended time after discharge. The Brain Injury Association (BIA) has chapters in every state that can help inform and support families. In the last decade, support groups for patients with TBI and their families have grown in size and number throughout the country. Unfortunately, TBI and its long-term effects (including behavior issues) are not well understood by society, which results in misconceptions about patient behavior and needs and often creates fear and mistreatment for many TBI survivors.
Living with a Brain Injury
Because of the advances in emergency medical systems during the past 20 years and because of the current state-of-the-art trauma centers with specialists and new technology, patients who would have died at the scene from a head injury are surviving and living a normal life expectancy. These individuals, however, are not normal. They live each day in communities across the country and struggle with their lifelong disability and cognitive impairments that often lead to early dementia, a shortened work life, the need for early retirement or disability pay, and premature aging with an early onset of medical problems. This population may be at higher risk for Alzheimer’s disease and other types of dementia. They are also at a higher risk for sustaining a fall and other injury if their home has not been evaluated and equipped with equipment and safety devices that enable them to live with their special needs. A patient who has lived at home may require early admission to a long-term care facility. The patient’s physical limitations and lack of endurance may qualify / classify him or her for disability and the need for expensive equipment (e.g., power wheelchairs, hospital wheelchairs) and for the services of physical or occupational therapists. Research on aging and brain injury is needed for patients and their families to successfully prepare them for the final years following a TBI.
Older Adult Considerations
Trauma is the fifth leading cause of death in older adults. The geriatric population (aged 65 years and older) has the second highest TBI incidence of all age-groups. The most common causes of TBI in the older are falls and motor vehicle crashes (MVCs). Older patients are more likely to develop chronic subdural hematomas (SDHs) and experience secondary injury than are their younger counterparts. Indeed, intracranial bleeding in older adults may occur even with minor head trauma due to the cerebral changes associated with aging.
Although TBI is not uncommon in older adults, the diagnosis is often complicated by an atypical presentation. For example, headache is the classic sign of SDH, yet in older adults it is often not a complaint. The presentation of an SDH is delayed weeks or even months, and unfortunately the insidious onset may be attributed to the normal aging process. Chronic SDHs are tolerated better by older adults because of the brain atrophy associated with aging. As the brain decreases in size, the space within the cranial vault increases.1,2,18 Therefore a hematoma can collect over time without obvious changes in neurologic status until its size is sufficient to produce a mass effect.
The assessment and management of older patients should follow the same algorithm as the care of younger TBI patients. The goals of treatment should focus on returning to the patient’s preinjury functional status and future quality of life. It is important to realize that the metabolic, anatomic, and psychosocial changes associated with aging may influence the assessment and care of the older patient with TBI.14 Injuries that are relatively survivable in younger adults can lead to complications and life-threatening events, including death, in older adults. Thus, in addition to hospital care, nursing interventions should also focus on injury prevention.
Environmental assessments, fall-risk profiles, and appropriate prostheses, assistive devices, and therapies can reduce the older patient’s risk for TBI related to falls. A rehabilitation focus that includes an acute-phase prevention of complications should be initiated as soon as the injury is discovered and should be continued throughout the course of recovery.
CONTINUUM OF CARE
Home Care / Rehabilitation
The rehabilitation phase of care for the patient with TBI begins at hospital admission. Acute inpatient admission to the rehabilitation unit is a milestone in the patient’s recovery and is a period of intense work by the patient to complete the daily schedule of therapies. The following are the goals of rehabilitation:
The Ranchos Los Amigos Scale of Cognitive Functioning is used as the basis for ongoing assessment of the patient in rehabilitation (see Table 13-2). The patient’s neurologic status and Glasgow Coma Scale (GCS) score are checked once or twice a day. Cognitive rehabilitation of the patient with a closed head injury requires a dedicated multidisciplinary effort.2
The patient should be observed and monitored for postconcussion syndrome (PCS). This condition is most commonly associated with mild TBI but can be seen after any form of TBI. There is no specific treatment for PCS, but it includes neurobehavioral therapy, rehabilitation, and medication.
The symptoms of a TBI may last as long as 6 months postinjury, but it is not unusual for someone in an intellectually demanding role to have significant symptoms for a year before returning to normal. (See RH1550 for more information on comprehensive rehabilitation.)
High-Risk Nursing Diagnoses
Impaired
physical mobility
Interventions for the patient with impaired physical mobility include the following:
Complications of impaired mobility include prolonged spasticity, contractures, and heterotrophic ossification (HO). HO involves the deposition of bone around the major joints and has the potential to cause a frozen joint and a functional loss of the use of the extremity.
Disturbed
thought processes
Using the behaviors outlined on the Ranchos Los Amigos
Scale of Cognitive Functioning, a care plan can be designed to decrease sensory
overload. The plan may include the following:
This program focuses on five core deficit areas:
Risk
for injury
Unpredictable and eccentric behavior is often seen in a
patient with TBI when arousal occurs. Behaviors include the following:
Interventions include controlling the environment by placing the patients in a quiet room, providing consistent caregivers, maintaining a strict schedule, and avoiding loud noises (radio, television), confusion, and too many visitors. Medications include haloperidol (Haldol) and lorazepam (Ativan). Sensory stimuli should be meaningful to the patient and presented in a structured format, because he or she has poor insight and judgment and requires careful monitoring. The use of restraints is discouraged unless no other avenues of preventing harm are successful.
Case Management Considerations
Case managers usually become involved with a TBI case when it becomes clear that the discharge plan will be complex and complicated. The exception is the case manager who becomes involved in the coordination of services and medical care for a patient who has problems from a concussion beyond 6 to 12 months. Almost half of all individuals recovering from a concussion experience symptoms afterwards, but fewer than 10% experience disabling symptoms that actually intensify instead of resolving. To help the individual return to work or school, a case manager can facilitate evaluation by a specialist for diagnostic studies, neuropsychologic testing, and treatment. Testing may include the following:
The goals of cognitive and behavioral rehabilitation after TBI are to enhance the patient’s capacity to process and interpret information and to improve his or her ability to function in all aspects of family and community life.27 Restorative training focuses on improving a specific cognitive function, whereas compensatory training focuses on adapting to the presence of a cognitive deficit. The case manager should be aware that these recommendations include the following:
The case manager assessment includes a thorough patient assessment and chart review, interviews with family members and members of the health care team and, in many instances, an evaluation of the patient’s home. Placement of the patient following hospitalization and inpatient rehabilitation is the first consideration. If the patient is in a persistent vegetative state or coma, a decision must be made for institutional care versus home care with 24-hour caregivers.
Case managers should be aware and review the 2000 Medical Rehabilitation Standards for Brain Injury Programs of the Commission on Accreditation of Rehabilitation Facilities. These standards cover rehabilitation programs, outpatient medical rehabilitation, home and community-based programs, long-term residential services, and vocational services. Through a case management approach, the CARF program addresses the following24:
The most prevalent impairment subsequent to a brain injury are severe cognitive deficits. With this awareness, a plan of care is developed with the health care team, patient and family members, and approval of the payer. Realistic short- and long-term measurable goals are included. Once approval has been received, the case manager implements the plan in a cost-effective manner to ensure continuity of care, monitors patient compliance, and includes patient and family satisfaction with the plan. The goal is functional restoration, compensatory training, prevention of complications, and avoidance of rehospitalization. The responsibility of the case manager may also include provisions for patient transportation, physician visits, and therapy sessions. Follow-up case management includes arranging for caregivers with appropriate home visits to provide wound care and dressing changes, medications, and nutritional evaluation, with frequent written reports from all members of the home health team.
Issues for the case manager to address include inappropriate client behavior that may interfere with social relationships and interpersonal relationships that could cause rejection by the spouse, relatives, friends, and associates. Sexuality and inappropriate sexual behavior can be another disturbing consequence of TBI. The use and abuse of drugs and alcohol may have contributed to the cause of the head injury and may also be a significant problem after discharge from the hospital or rehabilitation center. The need for a very consistent and structured lifestyle may create problems within a family unit. After TBI some individuals experience altered sleep patterns (e.g., napping versus sleeping at night, wandering during the night) that require 24-hour supervision. Quality of life issues are some of the more difficult challenges in case management.
The patient and family should be provided with a 24-hour telephone number to call for emergencies following TBI (with the understanding of what constitutes a medical emergency). The consequences of TBI may be lifelong, and the patient may require lifelong services. Preventing a second TBI requires care and injury prevention by all members of the team (and teaching for the family).
CONCLUSION
TBI affects 2 million people per year. The cost is staggering, and the outcome can be devastating. In a time when allocation of limited resources is a growing reality, the care of this population needs to be continually reevaluated, organized, cost-effective, and individualized. Nursing care of the patient with TBI is both challenging and complex. Clinicians must carefully consider how interventions affect patients. Care of the TBI patient is an area in which patient condition and response to care truly dictate the methods of nursing practice. Advanced technologic interventions, new pharmacologic agents, and research have improved the diagnosis and treatment of TBI. This has resulted in an increase in the number of survivors and has helped to reduce disability significantly. As scientists develop modalities for neuronal regeneration and repair, neuroscience nurses will play a key role in the patient’s return to functional independence.
American Association of Critical Care Nurses
E-mail: info@aacn.org
American Association of Neurological Surgeons
E-mail: info@AANS.org
http://www.neurosurgery.org/aans
American Association of Neuroscience Nurses
E-mail: info@aann.org
American Association for Surgery of Trauma
American College of Surgeons Committee on Trauma
American Trauma Society
(800) 556-7890
Brain Injury Association
105 N. Alfred Street
Alexandria, Virginia
(800) 321-7037
Brain Trauma Foundation
523 East 72nd Street
New York, NY 10021
(212) 772-0608
Copies of their publications are available:
Guidelines for the Management of Severe Head Injury
Guidelines for Prehospital Management of Traumatic Head Injury
Epilepsy Foundation of
America
(800) EFA-1000
{kind=link}
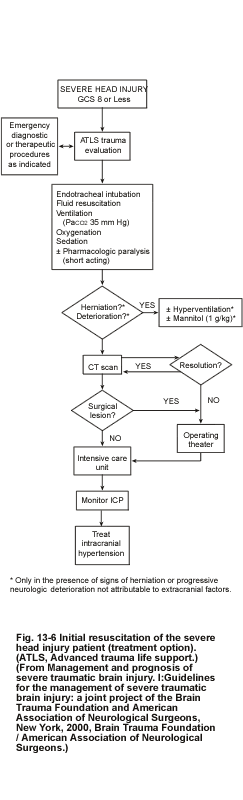{kind=link}